
The Fallacy of PCR Testing
Why a positive PCR result does not necessarily mean you have COVID-19

“In view of the current scientific evidence, this test alone proves to be incapable of determining, without a reasonable margin of doubt, that such positivity corresponds, in fact, to a person's infection with the SARS-CoV-2 virus…”
Judgement of the Lisbon Court of Appeal – Proc. 1783/20.7T8PDL.L1-3 – 11 Nov 2020 (English translation) (Original)
Introduction
Cases of COVID-19 are most commonly determined using a technology called polymerase chain reaction (PCR). Many people seem to be under the impression that a positive PCR result is equivalent to a case of COVID-19. However the evidence to support this assertion is lacking, and in fact there exists substantial evidence that PCR test results cannot be relied upon to determine infection with COVID-19. I will explain how PCR works and why claims of it being a “gold standard” for diagnosis of COVID-19 rest on shaky ground. We will see what the inventor of the technology had to say, as well as a contemporary expert’s opinion, we’ll examine how things can go wrong with the interpretation of PCR results, how disease prevalence affects test accuracy, the occurrence of pseudo-epidemics, court rulings, and more.
The polymerase chain reaction (PCR) technique was invented in 1983 by American biochemist Kary Mullis. It enables researchers to take a very small piece of DNA and rapidly copy it millions or billions of times, increasing the amount up to something that can be measured and studied. Previously copying DNA like this would take a team of scientists weeks or months but now it could be done in a few hours by a single technician. The New York Times described PCR as “highly original and significant, virtually dividing biology into the two epochs of before PCR and after PCR.”
PCR forms the basis of many processes in the fields of biochemistry and molecular biology, and there are many different types of, and ways to perform PCR. In the context of COVID-19 testing, the relevant type of PCR is:
Reverse transcription quantitative real-time PCR or RT-qPCR for short.
It’s a mouthful so let’s break it down.
Real time means just what you think it means, the results are available to view in real time as the experiment progresses.
Quantitative means that it is measuring the amount of the target DNA, showing whether there is a little or a lot, as opposed to simply detecting the presence of said DNA.
Reverse transcription is the process of converting RNA into complementary DNA or cDNA. Since SARS-CoV-2 is a single-stranded RNA virus, it’s genetic material needs to be converted into cDNA in order to amplify it using the RT-qPCR process.
(The abbreviation of RT-qPCR is a little confusing. The RT stands for “reverse transcription”, not “real-time”. The qPCR actually stands for “real-time quantitative PCR”. I know it’s weird but there you go.)
So RT-qPCR is a process that converts the RNA of SARS-CoV-2 (or whatever virus you’re looking for) into DNA, amplifies it, measures it in real time, and tells you how much genetic material was in the sample, if any. Because PCR works in this way it doesn’t give you a binary positive/negative result. Instead it outputs a graph and requires interpretation by a professional as to whether the result is indicative of an infection. See an example below:

PCR copies DNA in cycles. Every cycle doubles the amount of DNA present. Typically PCRs run for about 40-45 cycles. Technicians use something called a quantification cycle (Cq) or cycle threshold (Ct) to determine whether a sample is deemed positive or negative. (The terminology varies, some use Cq and some use Ct but they mean the same thing. I will use Cq because this term is proposed in the MIQE guidelines which are mentioned below, however many people still use Ct and I preserve the original language when quoting them.) If the sample crosses the Cq it means there is enough present to be considered positive. If it only takes a few cycles to cross the threshold it indicates a larger amount of target DNA, if it takes more cycles to get there, it indicates less DNA since it needed to be replicated more times. This means a Cq value is inversely related to the amount of virus detected. Low Cq means more virus, high Cq means less virus.
However, where the Cq should be is not an exact science. Choosing different Cq values will have different trade-offs. If you choose a Cq value on the lower end you will be more likely to get positive results for people who are actually infectious, but may miss some cases that were just above the cut-off. If you choose a Cq value on the higher end you will catch more infectious cases but may also misdiagnose noninfected people with a positive result. Essentially, do you want less false-positive results or less false-negative ones?
The U.S. Food and Drug Administration neatly summarises the problems with each (in the context of antigen testing but the principle is the same):
False-negative results may lead to delayed diagnosis or inappropriate treatment of SARS-CoV-2, which may cause patient harm including serious illness and death. False-negative results can also lead to further spread of the SARS-CoV-2 virus, including when presumed negative patients are grouped into cohorts in health care, long-term care, and other facilities based on false test results.
False-positive results could lead to a delay in the correct diagnosis and the initiation of an appropriate treatment for the actual cause of patient illness, which could be another life-threatening disease that is not SARS-CoV-2. False-positive results could also lead to further spread of the SARS-CoV-2 virus when presumed positive patients are grouped into cohorts based on false test results.
As a famous economist once said: “There are no solutions, only trade-offs.” Deciding on a Cq value is a balancing act with no definitive solution.
Dead or Alive?
An important point to understand is that PCR does not differentiate between “live” and “dead” virus, it only detects the genetic material. To be more precise, it does not distinguish between infectious and non-infectious virus. You can carry viral RNA fragments in your system without being infected. These would be “dead” bits of nonreplicating virus, however they are still able to be detected with PCR because PCR is detecting the genetic sequence that these bits of RNA share. Some people have tested positive for up to three months after having COVID-19 because the test is still detecting these RNA fragments.
This seems to call into question the ability of PCR to determine infection. If you can still get a positive result for months after the illness, is it really up to the task? PCR inventor Kary Mullis has publicly stated in no uncertain terms what the answer to this question is. Here’s what he said:
“It’s just a process that’s used to make a whole lot of something out of something. It doesn’t tell you that you’re sick and it doesn’t tell you that the thing you ended up with really was gonna hurt you or anything like that.”
Kary Mullis, awarded the 1993 Nobel Prize in Chemistry for his invention of PCR (Source of quote)
This quote is taken from the clip below:
In the same clip he states:
With PCR, if you do it well you can find almost anything in anybody. It starts making you believe in the Buddhist notion that everything is contained in everything else. Cause if you can amplify one single molecule up to something that you can really measure, which PCR can do, then there’s very few molecules that you don’t have at least one single one of in your body. So that could be thought of as a misuse of it, just to claim that it’s meaningful.
So the inventor of PCR technology says that it doesn’t tell you if you are sick. Though that was in 1993, perhaps the technology has progressed since then passed what Mullis thought it capable of. Unfortunately Mullis passed away in 2019 — before the COVID-19 pandemic began — so for more recent insight we will turn to Stephen Bustin, a world-renowned expert on quantitative PCR and author of many works on PCR including the MIQE guidelines and a book entitled A-Z of Quantitavive PCR which has been called “the bible of qPCR.” The MIQE guidelines standardise the information that technicians need to report when performing real-time PCR experiments and is the fifth most cited paper in Clinical Chemistry with over 1,700 citations. He is the head of the Molecular Diagnostics Unit at Anglia Ruskin University and specialises in “translating molecular techniques into practical, robust and reliable tools for clinical and diagnostic use”, which is precisely what we are concerned with.
So what does Bustin have to say about RT-qPCR? Well in an interview in February 2021, with Eric Coppolino for Planet Waves FM he said this:
You have to distinguish between the presence of target and the presence of […] virus. Just because you detect a fragment of RNA doesn’t mean you’ve got infectious virus present.
And the problem here is, that there are no certified standards […] that tell us what the Cq actually means in any particular experiment. And if you look at my paper that I’ve published in Scientific Report we’ve tried to put in a standard that we’ve quantified, but that still only tells you that there are 10 copies, or 5 copies, or 100 copies. We then need to relate that to some kind of clinical context to know whether that cycle threshold of 30 say, does actually mean there is infectious virus. And that has not been done yet.
So all you can say at the moment with these tests is that if you take a test and you have a positive result, it is likely that you have virus present. In order to say whether this is likely to be infectious you would need to take the test again a day or two after you’ve had the first test. Because if it really is in the early stages on infection then you would get a decrease in the Cq. If you at the late stage on infection when you are no longer infectious then it will either disappear altogether or the Cq comes down from say 25 to 30 or 35.
So that’s the qualitative aspect of it. People try and use it quantitatively, particularly to discuss viral load, and you just cannot do that at the moment. We have no idea what a Cq means in terms of viral load. And then we can’t extrapolate from that into a clinical context i.e whether this person is infectious or not. [My emphasis.]
Planet Waves FM interview with Stephen Bustin, conducted by Eric F. Coppolino, 1 Feb 2021. (Quoted dialogue begins at 9:20)
Seems that not much has changed in regards to PCR’s ability to diagnose infection. It is a very powerful lab tool that can detect and amplify even a single molecule, a very impressive piece of technology. However this does not necessarily mean it lends itself to clinical diagnosis of disease which requires a combination of testing, medical examination and consideration of medical history. As the author of a 2022 paper titled Diagnosis: Fundamental Principles and Methods stated:
First, it has been said that “one’s ears are the best diagnostic tool,” with evidence from a patient’s history often trumping complex and expensive special investigations. More emphasis on the clinical history and examination is helpful before special investigations are requested.
It is unlikely that the hypothetical certified standards that Bustin referred to have emerged since he was interviewed in 2021. Scientists are still having trouble following his MIQE guidelines which were published in 2009. In 2017, eight years after their publication Bustin published two papers admonishing the state of RT-qPCR reporting. One paper states:
Despite the impact of the minimum information for the publication of quantitative PCR experiments (MIQE) guidelines, which aim to improve the robustness and the transparency of reporting of RT-qPCR data, we demonstrate that elementary protocol errors, inappropriate data analysis and inadequate reporting continue to be rife and conclude that the majority of published RT-qPCR data are likely to represent technical noise.
The other reads:
It is obvious that this situation is not going to improve until journal editors, in particular, begin taking this egregious, I am tempted to say scandalous, situation seriously and start to appreciate first, that the majority of peer-reviewed publications utilising qPCR-based methods are seriously flawed
A survey of participants revealed that whilst 72% and 68% respectively, of individuals carrying out RT-qPCR experiments thought the technique was simple and reliable, only 6% were aware of the guidelines. Regrettably, this also applied to those describing themselves as “expert” users, with a disappointing 13% awareness. Most disheartening was that none of the novice users had heard of the existence of the guidelines.
When guidelines have been out for eight years and only 6% of technicians are even aware of them, while a world-renowned expert says the majority of data are probably just “technical noise”, we have a problem. A few years later the COVID-19 pandemic occurs and we seen an explosion in the number of RT-qPCR tests being performed. With the state of RT-qPCR reporting being as abysmal as it was, in addition to the huge influx of inexperienced technicians into an area where the majority of people produce technical noise while under the illusion their work is easy and reliable; how much trust can we really place in the results of PCR COVID-19 testing?
To give you an idea of what it takes to perform real-time PCR you can watch Dr Lexa Scupham’s excellent video demonstration.
It’s important to note that it’s not necessarily the RT-qPCR lab technique itself that is at fault, but the interpretation of the results. Nowhere is this most exemplified than in quantification cycles and the reliance upon them to determine active infection.
“RT-PCR which everyone thinks is easy, is particularly prone to problems.”
Stephen Bustin, lead author of the MIQE guidelines ( Source of quote: The Infectious Myth - Stephen Bustin on Challenges with RT-PCR — Apr 14, 2020 — Quoted dialogue at 51:00)
Quantification Cycles
Researchers from England have performed a study on the relationship between Cq (Ct) values and culture positivity. In other words, they looked at which samples they were able to grow in a lab and compared that to the Cq values. This helped them determine how likely a given Cq is to represent “live” infectious virus.
(Remember Cq = Ct. Both refer to the exact same thing.)
The results are displayed below:
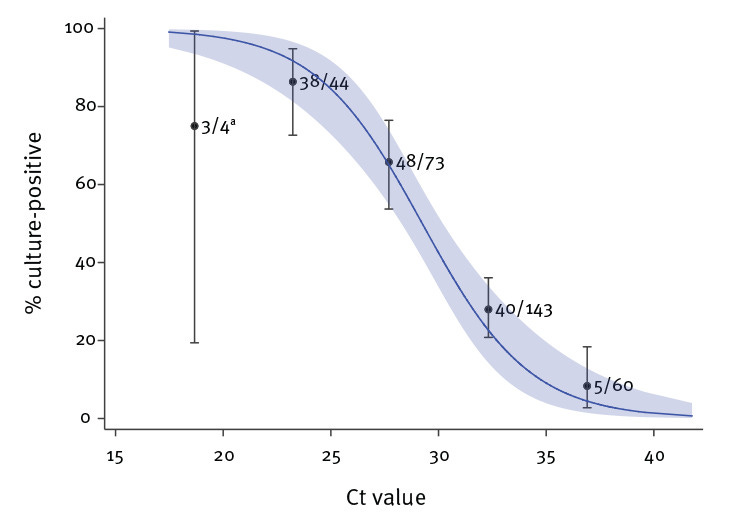
From this data we can clearly see that as the Cq value increases, the chance of a sample representing infectious virus decreases. Once you reach the high 20s the accuracy drops below 50%. Anything below 20 is approaching 100% accuracy. One might argue that a reasonable Cq to define an infectious person would be somewhere under 25, though this is certainly up for debate. What seems less up for debate is using a Cq over 30 or 35, at which a person has below a 50% chance of being infectious.
High Cq values produce false positives
Just to drive the point home, below is a list of evidence that demonstrates high cycle thresholds, especially above 35, produce false positives:
“Careful interpretation of weak positive NAAT [nucleic acid amplification test] results is needed, as some of the assays have shown to produce false signals at high Cq values.”
“If you get a cycle threshold of 35 or more, the chances of it being replication competent are miniscule.”
Dr. Anthony Fauci, former Chief Medical Advisor to the President of the United States and Director of NIAID (Source of quote)
“At Ct = 35, the value we used to report a positive result for PCR, <3% of cultures are positive.”
Rita Jaafar, Sarah Aherfi, Nathalie Wurtz, Clio Grimaldier, Thuan Van Hoang, Philippe Colson, Didier Raoult, Bernard La Scola, Correlation Between 3790 Quantitative Polymerase Chain Reaction–Positives Samples and Positive Cell Cultures, Including 1941 Severe Acute Respiratory Syndrome Coronavirus 2 Isolates, Clinical Infectious Diseases, Volume 72, Issue 11, 1 June 2021, Page e921, https://doi.org/10.1093/cid/ciaa1491
“If someone is tested by PCR as positive when a threshold of 35 cycles or higher is used (as is the rule in most laboratories in Europe and the US), the probability that said person is infected is less than 3%, and the probability that said result is a false positive is 97%.”
Judgement of the Lisbon Court of Appeal – Proc. 1783/20.7T8PDL.L1-3 – 11 Nov 2020 (English translation) (Original)
“Following SARS-CoV-2 infection, low amounts of SARS-CoV-2 RNA with high Ct values (e.g. more than 35 cycles) can be detected for several months. Studies using viral culture methods have shown that this represents non-infectious shedding of nonviable viral fragments.”
What Cq are we using?
Unfortunately many places around the world have been using Cq values that are way too high. The evidence below demonstrates 35 and even 40 are common thresholds used to define a positive PCR result:
US CDC guidelines instruct technicians to use a Cq of 40.
Researchers from Israel define a positive result up to a Cq of 40 in a 2022 paper.
The New York Times reports that most tests set the Cq at 40, a few at 37.
Post-market validation documentation defines a positive result for various assays up to Cq values of 38 and 40.
The Lisbon Court of Appeal states most laboratories in Europe and the US define a positive result up to 35 cycles.
Judgement of the Lisbon Court of Appeal – Proc. 1783/20.7T8PDL.L1-3 – 11 Nov 2020 (English translation) (Original)
Clearly such high thresholds are going to produce a large amount of false positives. This is confirmed by the New York Times:
“In three sets of testing data that include cycle thresholds, compiled by officials in Massachusetts, New York and Nevada, up to 90 percent of people testing positive carried barely any virus, a review by The Times found.”
It appears that what Bustin had written in 2017 still holds true in that the majority of RT-qPCR results are “technical noise” and cannot be relied upon. Especially when using such insanely high quantification cycle values. Even if we were to raise the threshold (lower the number) to a more reasonable level there are still difficulties with relying on Cq values to diagnose someone with an infection.
A 2023 paper notes:
Ct values from qualitative RT-PCR tests should not be used for clinical or epidemiological decision-making to avoid the potential for misinterpretation of the results.
Another from the same year states:
…regarding the assessment of transmission and infection control, studies investigating the correlation between CT values and infectious SARS-CoV-2 have shown conflicting results, suggesting the inappropriateness of using CT values to extrapolate and establish a cutoff value for virus infectivity and clinical significance.
Essentially, the Cq values used for COVID-19 testing were way too high, meaning the threshold was way too low for designating someone as an infectious COVID-19 case. But even if a more reasonable threshold is used, there still do not exist standards that would allow for the extrapolation of the PCR results into a clinical diagnosis or level of infectiousness. Even the chart above may not be enough to reliably diagnose a patient, especially since not all studies agree on the relationship between Cq and infectivity.
Of note here is that different PCR machines and different methods used in various laboratories around the world can yield different results. Thus, one lab’s Cq of 25 could be another’s 33, further complicating the process of standardisation that might allow for an accurate diagnosis of infectivity from RT-qPCR experiments.
According to the MIQE guidelines, reporting of Cq values with the results is essential in order for the results to be properly interpretable and yet many labs are simply returning a “positive” or “negative” result. Without knowing the Cq values it’s hard to say how likely those results are to be correct.
But wait, there’s more.
“Establishing a limit of detection based on Ct is dangerous because you can change your Ct simply by raising and lowering the threshold.”
Dr. Lexa Scupham (Source of quote 50:48)
Testing across time
One idea that Bustin noted in his interview with Eric Coppolino and which I have quoted above is that of performing a PCR experiment more than once and measuring the difference between the two results. If the number of cycles increases then you are likely at late stage of infection, if it decreases then you may be at the beginning of it as your viral load increases. As a document published by the English health department states:
Whilst high Ct values may be associated with reduced infectivity, a swab taken at a single point in time does not provide information about the trajectory or subsequent course of illness.
So one PCR test is not enough, we need two to help us determine infection, or at least, get more detailed and actionable results. We have just discussed the fallibility of using Cq values to diagnose infection however maybe with this time sensitive approach we could extract more reliable and helpful information. So are we doing this? Well judging by how this article has gone so far you can probably guess the answer.
A systematic review by Cochrane of 155 study cohorts looked at the accuracy of antigen tests. Of course if you want to assess the accuracy of a test you need to have something to compare it against. Since RT-PCR is apparently the “gold standard”, this is what was used to compare the antigen tests to. In the main findings of the paper the authors state:
Nearly all studies (91%) used a single RT-PCR result to define presence or absence of infection. [My emphasis.]
Coppolino: Every time someone gets a PCR positive the NYT and everyone else is calling that a confirmed case of Covid. I don’t understand what the confirmation is, there’s no split sample, there’s no resting, there’s no symptoms…
Butin: I guess if you definition of confirmed is… you’ve confirmed there is SARS-CoV-2 RNA there, that’s what I would say.
Coppolino: But they’re calling it a confirmed case of infection.
Butsin: [Awkwardly] Yeah… Ah.
Planet Waves FM interview with Stephen Bustin, conducted by Eric F. Coppolino, 1 Feb 2021. (Quoted dialogue begins at 27:44)
To sum up: we are using Cq values to define infection when arguably we should not be. And when we use Cq, we use values that are way too high making the majority of positive results false. On top of this we could be improving results by testing across time but 90% of studies don’t do this. Could this fiasco get any worse? Yes, actually it can.
How disease prevalence affects test accuracy
“Positive and negative predictive values are highly dependent on prevalence. False-negative test results are more likely when prevalence of disease is high. False-positive test results are more likely when prevalence is moderate to low.”
Something I don’t see discussed enough in relation to COVID testing is how the prevalence of the disease affects the accuracy of a test. This isn’t something that’s specific to COVID testing, it’s a consequence of mathematics.
Imagine you test a population of 100 people. The test is quite accurate with an accuracy rate of 99%, meaning only 1% of positive results will be false-positives. The prevalence of the disease is low at 1% of the population. Out of the 100 people tested, the test will pick up the 1 infectious person, however it will also produce 1 false positive result. Thus we will have 2 positive results. For any individual with a positive test the chance of actually having the disease is now 50%, one real positive and one false one. A seemingly high test accuracy has been reduced to no better than chance by the low prevalence of the disease.
For an in-depth explanation of this phenomenon watch Dr. Trefor Bazett’s video:
To give you an idea of how prevalent COVID is currently you can consult the graph below. (You may be reading this in the future in which case you can click on the graph to take you the Our World in Data website which should have the current figures.)
The global average for “confirmed” cases of COVID-19 (as of writing this in February 2024) is at 0.43 per million, which is 0.000043% of the population. For my country of Australia it’s currently at 42.23 per million which is 0.0042%. Even if we take the tallest peak in the graph which is France in January of 2022 it still only equates to 0.53% of people in France who are infected.
If even a test accuracy of 99% can be reduced to half with a 1% disease prevalence, what would happen with a test much less reliable and a disease rate even lower?

It’s worth pointing out that these case numbers are based on, you guessed it, positive PCR results. So how accurately they represent the number of COVID cases is highly questionable and using them to determine the prevalence of SARS-CoV-2 which is in turn is used to evaluate the accuracy of the test is somewhat of a circular exercise. However, given the high sensitivity of PCR and the extremely high Cq’s being used and it seems reasonable to conclude that lower case numbers are more likely to be accurate than higher ones.
Notice the subtext underneath the title of the graph: “Due to limited testing, the number of confirmed cased is lower than the true number of infections.” It’s unclear how Our World in Data know this to be the case and considering everything we have discussed so far this statement seems extremely dubious. As you will see in the section titled “History Repeating”, more testing doesn’t necessarily equate to more accurate numbers.
Court Rulings
You may recall the very first bit of text in this article was an excerpt from a judgement by the Lisbon Court of Appeal. Here it is again to refresh your memory:
“In view of the current scientific evidence, this test alone proves to be incapable of determining, without a reasonable margin of doubt, that such positivity corresponds, in fact, to a person's infection with the SARS-CoV-2 virus…”
Judgement of the Lisbon Court of Appeal – Proc. 1783/20.7T8PDL.L1-3 – 11 Nov 2020 (English translation) (Original)
In fact both the Lisbon Court of Appeal in Portugal and the Vienna Administrative Court in Austria have determined that PCR is not suitable for diagnosis.
The Lisbon case arose when four German tourists holidaying in Portugal were forced into quarantine for sixteen days based on a single positive PCR result. Only one of the four tested positive but the others were considered a “high infection risk” because of their proximity.
The court ruled their detainment to be illegal.
The judgement cites an article published in Clinical Infectious Diseases containing information that should be quite familiar by now:
It can be observed that at Ct = 25, up to 70% of patients remain positive in culture and that at Ct = 30 this value drops to 20%. At Ct = 35, the value we used to report a positive result for PCR, <3% of cultures are positive.
Emphasised was the fact that none of the claimants had been seen by a doctor which the judgement states “is frankly inexplicable, given the alleged severity of the infection.” … “A diagnosis is a medical act, the sole responsibility of a doctor.” This is an important point to drive home, a test by itself cannot diagnose a patient. A doctor may use a test to aid in their diagnosis but the diagnosis must come from a qualified human person, not from a piece of laboratory equipment. A test is used alongside physical examination and patient history, not instead of.
The Vienna Administrative Court echoes these findings in it’s ruling on the restrictions of gatherings, citing research finding no viral growth in samples with a Cq value over 24.
This judgment also agrees that “whether a person is sick or healthy must be determined by a doctor.” [Emphasis in original text]
It’s unfortunate that these court rulings have not had the attention they deserve in the media as they are powerful additions to the evidence base that shows RT-qPCR to be unsuited to diagnosing infection with SARS-CoV-2, while reminding us that a diagnosis cannot be performed by a piece of lab equipment which does not have access to a patients medical history, and cannot assess symptomatology or conduct clinical examination.
History Repeating
This isn’t the first time PCR technology has led us astray. In 2006, at the Dartmouth-Hitchcock Medical Center in New Hampshire a whooping cough (pertussis) epidemic had sprung up. An intern was coughing nonstop for two weeks and others around her began to cough as well. Widespread PCR testing was performed which showed 142 positive results for pertussis, staff were put on leave, and thousands were given antibiotics and a vaccine.
Some time later however, once a more definitive test had been performed — actually growing the bacterium in a lab — it was discovered that none of the samples contained the bacterium in question. Those affected by bouts of coughing were likely just experiencing a common cold variety. Faith in PCR had led to the creation of a pseudo-epidemic.
This is not an isolated incident either, Johns Hopkins epidemiologist Dr. Trish Perl told the New York Times that pseudo-epidemics happen all the time.
Infectious disease specialist Dr. Kathryn Kirkland said, “we have had a number of outbreaks where we believe that despite the presence of PCR-positive results, the disease was not pertussis.”
One of the problems is many of the symptoms are not unique to pertussis, things like persistent coughing and a runny nose can also be symptoms of a common cold. “Almost everything about the clinical presentation of pertussis, especially early pertussis, is not very specific,” Dr. Kirkland said.
Another problem was lowering the threshold of who was to be tested. Anyone with a cough got a PCR test. For those working with high-risk patients even a runny nose was enough to warrant a test. “Because we had cases we thought were pertussis and because we had vulnerable patients at the hospital, we lowered our threshold,” Kirkland explains.
This section is a summary of a New York Times article written by Gina Kolata in 2007. I recommend reading it if you want a fuller picture of what took place.
New York Times - “Faith in Quick Test Leads to Epidemic That Wasn’t” by Gina Kolata - 22 Jan 2007 (Archived 24 Oct 2015)
This is sounding all too familiar. Nonspecific symptomology, the lowering of thresholds; this all applies to COVID-19. Fever, coughing, muscle aching, sore throat, runny nose, fatigue, and loss of taste and smell are all symptoms of COVID-19 but could easily be symptoms of other respiratory illnesses. The lowering of thresholds has occurred on two fronts, the use of high Cq values that we have explored ad nauseum already, and the testing of anyone and everyone, including asymptomatic people, taking it a step further than Dartmouth-Hitchcock Medial Center who at least required a runny nose before testing.
So PCR has led to the creation of pseudo-epidemics in the past and PCR is the basis for COVID-19 statistics all across the globe. That raises the question: was COVID-19 a pseudo-pandemic? Or perhaps if that’s going too far we could ask: Has the reliance on PCR and high Cq values led to inflated numbers and thus created a warped perception of the true impact of the virus? I will not attempt to answer that question here, however I will state that given all we have discussed above this remains a distinct possibility, even a probability.
“It’s a problem; we know it’s a problem. My guess is that what happened at Dartmouth is going to become more common.”
Dr. Trish M. Perl, president of the Society of Health Care Epidemiologists of America (Source of quote)
Conclusion
Summing up what we’ve learned:
PCR is and important and game-changing technology in the fields of molecular biology and biochemistry. It is extremely sensitive and can detect miniscule amounts of DNA, copying it millions or billions of times.
There do not exist reliable standards for the interpretation of Cq values, and the extrapolation of them into a clinical diagnosis of infection. A diagnosis should be performed by a medical professional, not by PCR alone.
PCR it not easy to do and requires interpretation by a professional. Even many people who claim to be experts in PCR are not aware of the MIQE guidelines, do not publish the relevant information with their results, and are producing technical noise.
Cq values used to determine a positive result are often way too high, thus being an extremely low threshold for a positive result, creating up to 90% false-positives.
Testing across time could improve reliability of results however 90% of studies do not do this.
Low disease rates will reduce the accuracy of any test. Rates of COVID-19 infection are low.
PCR has led to the creation of pseudo-epidemics in the past.
Two court decisions have ruled that PCR testing is not adequate for determining whether an individual is infectious or not.
Given all this it is difficult to see why one should put any stock in PCR results to determine infection, either on an individual or population level.
Things get a little more real when we consider the fact that PCR results are being used to force people into quarantine. We can argue about whether it’s ethical to force people with COVID-19 into quarantine in the first place, but if the test we are using to do so is not reliable then it seems straightforwardly wrong to violate an individual’s right to freedom of movement based on such a test.
During the pandemic it was commonplace to force people into quarantine based on the results of this flawed method of diagnostics. One particularly egregious example of this comes from the Howard Springs quarantine facility in Australia where Northern Territory resident Hayley Hodgson was forced into quarantine for being a close contact of someone with a positive PCR result. Investigators tracked her down and police escorted her to the facility where she was forced to stay for fourteen days despite testing negative three times. Because of this forced isolation she lost her job. She never even had COVID-19. This is just one example of how overreliance on a faulty test can damage lives. Watch her interview with UnHerd below.
This widespread reliance on PCR alone to determine infection, guide policy, and force people into quarantine camps is setting a dangerous precedent.
You may recall this quote from above, I think it bears repeating:
“First, it has been said that “one’s ears are the best diagnostic tool,” with evidence from a patient’s history often trumping complex and expensive special investigations. More emphasis on the clinical history and examination is helpful before special investigations are requested.”
By relying solely on this molecular test we are moving away from clinical examination. People are being diagnosed with a disease and denied their rights without even being examined by a doctor. Moving away from expert human judgement to the reliance on machines is a dangerous precedent. Especially when said machines which are naively viewed as much more reliable and capable than they in fact are. This unprecedented reliance on PCR is removing clinical examination and symptomatology from the diagnostic process. If we want to bring back trust in the medical field we need to bring back the humanity.
I will leave you with this moment from David Crowe’s interview with Stephen Bustin:
Crowe: If you have a nice shiny machine and you put samples in it and the machine does everything for you and at the end it produces a graph or a number or something like that, does that lead you to believe that it’s simpler and more precise than it might actually be?
Bustin: Yes, absolutely.
The Infectious Myth - Stephen Bustin on Challenges with RT-PCR — Apr 14, 2020 — Quoted dialogue at 51:08)